SHAPESHIFTER
I have to make you sick to make you well,
The oncologist says, five months
we’ll scour each cell of your abdomen clean.
INTRAPERITONEAL CHEMO
It always burns, multiples thousands of bone splinters
stinging cells, murdering nerves, dulling
my mind, my spine alive, a drawn bow
aimed at heaven, sprouting agony’s three stingy feathers.
Both from Refugee; poems by Pamela Uschuk
When I first learned that our friend Pamela Uschuk had ovarian cancer, I despaired for her life. Ovarian cancer is one of the worst killers. By the grace of God, and the Mayo Clinic, she is still alive and well 10 years later.
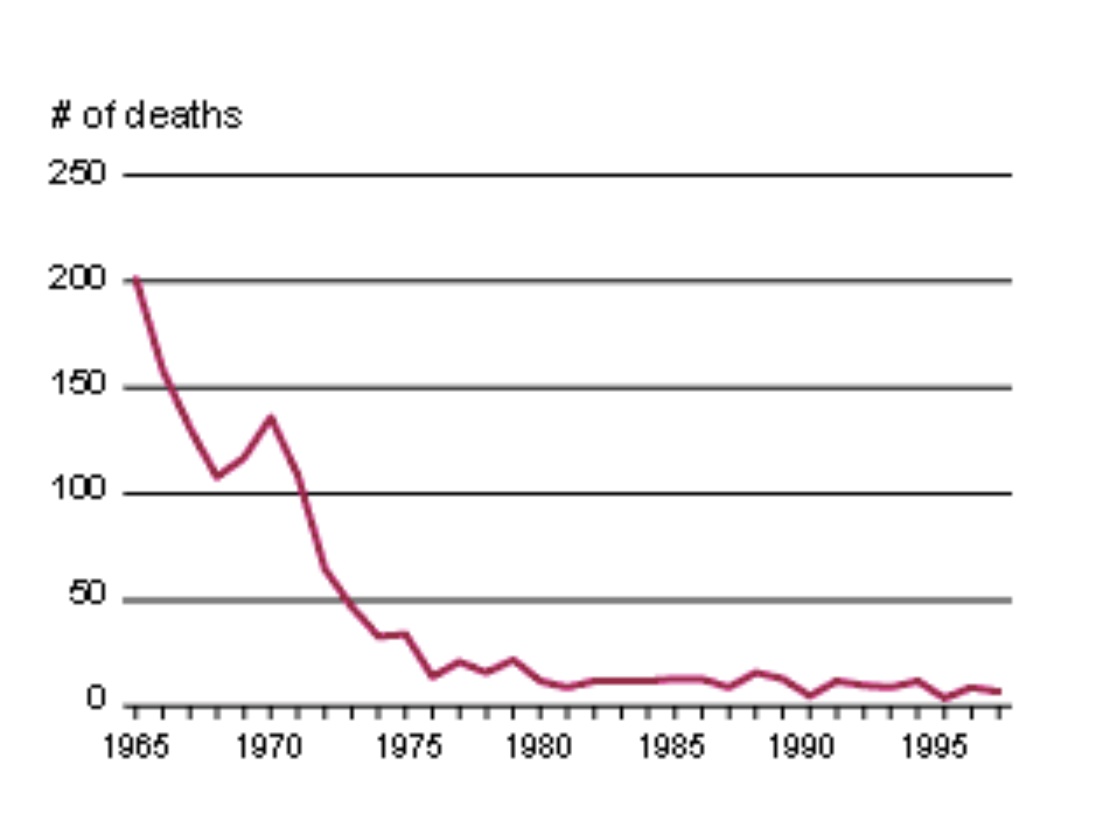
Unfortunately, there is no screening test, like the Pap smear, for this terrible disease. Ovarian cancer has usually spread widely by the time that it is detected, so heroic treatment is required. Despite medical advances, most women who get ovarian cancer are killed by it.
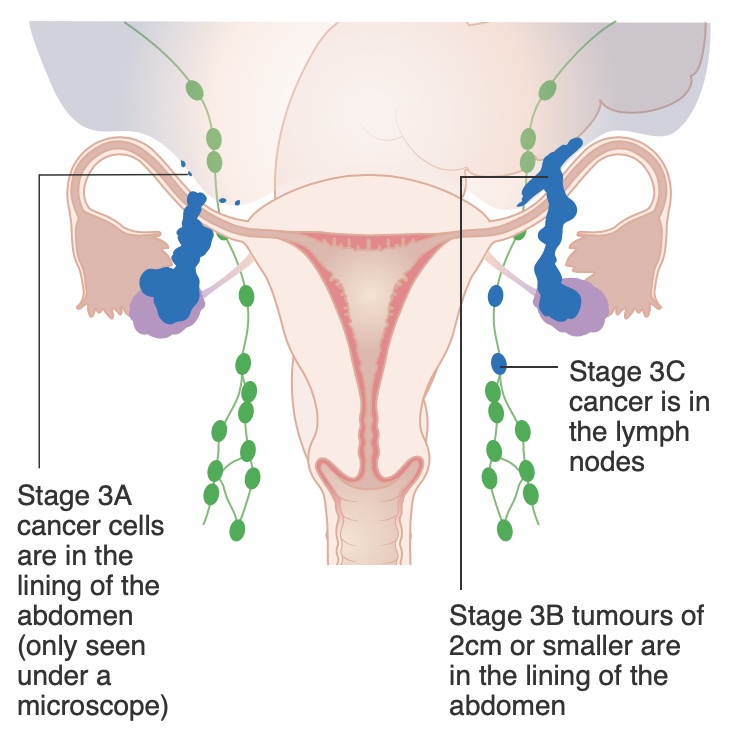
Mysteriously, the risk of getting ovarian cancer is reduced by using birth control pills, by tubal ligation or by hysterectomy. Even more puzzlingly, about a decade ago it was discovered that most ovarian cancers actually start in the Fallopian tubes.
Ovarian cancer is not that rare—about 1 in 80 women will develop it. Some women are at higher risk because they carry a genetic mutation such as BRCA, but they only account for about one tenth of the people who develop this disease. Pamela was at normal risk; she is BRCA negative.
Now, rather than just blocking a woman’s tubes to prevent pregnancy, it is recommended to consider removing the tubes entirely (salpingectomy). The final word isn’t in because the recommendation is too new, but bilateral salpingectomy has the possibility of preventing hundreds of cases of ovarian cancer, saving many lives annually!
If a woman has a planned Cesarean with what she intends to be her last child, why not have a salpingectomy at the same time? After all, her tubes are exposed and this procedure only adds 5 minutes to the surgery.
Regrettably, that may not be possible in some hospitals under Catholic control. They must abide by the “Ethical and Religious Directives for Catholic Health Care Services” of the United States Conference of Catholic Bishops. This document states:
“Direct sterilization of either men or women, whether permanent or temporary, is not permitted in a Catholic health care institution. Procedures that induce sterility are permitted when their direct effect is the cure or alleviation of a present or serious pathology and a simpler treatment is not available.”
This statement has unintended consequences. Many women have hysterectomies in Catholic hospitals because the simpler, safer and less expensive tubal ligation is prohibited. Worse, this policy leads to unplanned pregnancies and abortions. Remember, the most effective way of preventing abortions is with effective contraception!
Of course, there is the option for the new mother to go to another hospital at a later time for her tubal surgery, but that means a second anesthesia, additional cost, plus more pain and recovery time. What mother wants to leave her newborn child and not be able to breastfeed?
All healthcare institutions should endeavor to prevent illness and death. A study examined the number of women having tubal ligations at the time of cesarean birth and calculated that over 900 cases of ovarian cancer and 550 deaths every year in the USA could be prevented by doing salpingectomies for women who want sterilization at the time of cesarean.
Let’s look at this issue from a different viewpoint. What if it had been shown that vasectomy decreased the risk of testicular cancer (it doesn’t, unfortunately). Do you think that the Catholic patriarchy would deprive their priests and other men of this potentially life-saving surgery?
Preventing sterilization, especially salpingectomy, at the time of cesarean is a case of religious doctrine standing in the way of good medical care.
© Richard Grossman MD, 2022