The Cairo Conference “Programme of Action” includes a statement that all people should have the right to decide freely and responsibly the number and spacing of their children. Unhappily, many people have been forced to follow the old adage “the rich get richer and the poor get children”.
Fortunately, this adage has been disproven in at least 5 countries where voluntary Family Planning (FP) has been made accessible to all, with little regard to income. Brazil, Ecuador, Egypt, Ethiopia and Rwanda were chosen for study because they represent different societies on different continents. 196 policies affecting the availability of FP services were identified in these countries from 1961 to the present, and the effect was described in a 2024 analysis. The progress in the availability of high-quality FP is amazing in all five of these countries!
The genocide in Rwanda was 30 years ago. Hunger was a factor that led to neighbors killing neighbors. People in many places in this largely agrarian society were not able to produce enough food to keep away hunger. Contributing factors included land degradation and rapid population growth; there was no violence in areas where people had at least 1500 calories of food per day. The average American eats almost twice that amount!
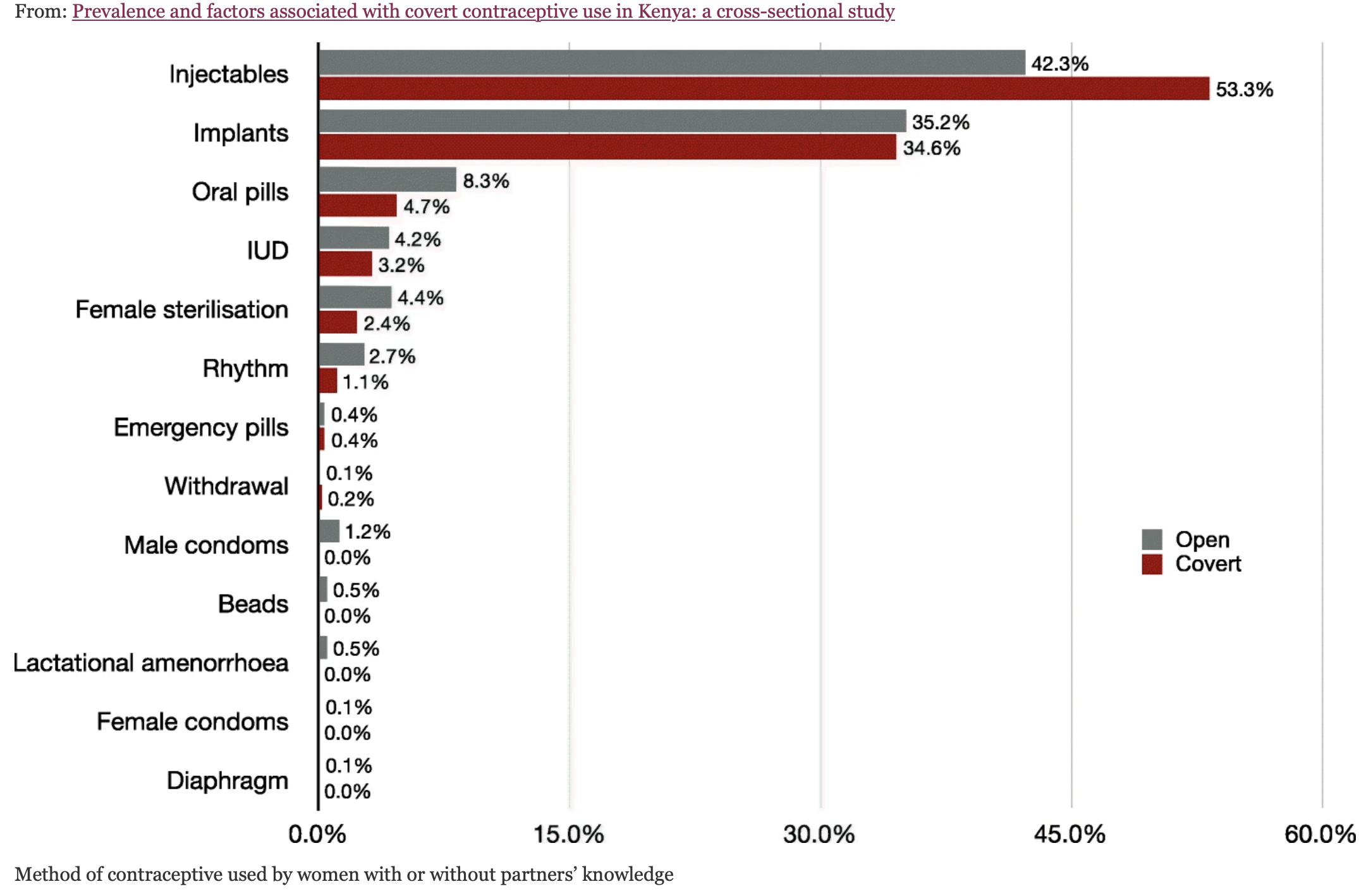
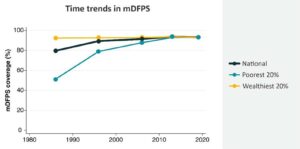
Back in the year 2000, few low-income people in Rwanda had access to modern FP. The country was largely Roman Catholic, which forbad modern FP and relied heavily on unreliable rhythm for birth spacing. Then, in 2005, the government started supporting a more effective method of natural FP, the Standard Days Method (SDM). The Church approved of SDM and it became popular. It is simple and is up to 95% effective—if used properly. Only 5 years after its introduction, the proportion of the poorest couples using effective contraception had risen to half!
The year 2005 also marked a presentation that changed attitudes in the Rwandan Parliament. The RAPID Model is a computer-based tool that stakeholders can use to demonstrate the effect of rapid population growth on different sectors, and the benefits of FP programs. The model demonstrated how FP can reduce mortality, improve health and increase the availability of women in the workforce. Rwanda has taken advantage of that benefit: almost 2/3 of members of parliament are women—the highest percentage of any country! RAPID also showed the economic benefits of FP—for every dollar spent on contraception, the government would save four. To quote a minister of health, “family planning is a tool of development.”
Since the five countries have different conditions and customs, each approached the need to slow population growth with different policies. For instance, the literacy rate is low in rural Egypt, so they used TV to get across FP messages. Ethiopia established primary health care for all—including contraception. Brazil focused on preventing adolescent pregnancies by improving sexuality education and facilitating access to FP for teens. In 2008 a change in Ecuador’s constitution named health care as a right, and ensured that women could make their own decisions about FP. Rwandan policies have already been discussed. It is remarkable that all 5 countries established policies that increased use of effective FP—and in 3 of the countries, there is equity between rich and poor in their use of FP.
Although each of these countries has its own policies and areas of focus, they all received help from the US government and from other rich countries. Nongovernmental agencies, such as the Gates Foundation, also provided expertise and resources. It is wonderful that all 5 of these countries did what they could to make family planning services available to all.
© Richard Grossman MD, 2024