![]()
I was walking down the street in Mountain View, California when I noticed a man coming toward me wearing a white T-shirt with small black lettering: “SEEDLESS”. I wonder if he was advertising his vasectomy?
Vasectomy motivators in Northern Sumatra use humor in their presentations to men about vasectomy. Perhaps they should wear shirts with “KESIP” (Indonesian for “seedless”) on them! From what I can tell, these motivators need all the help they can get, since very few men get vasectomies in Indonesia. However, Indonesian husbands tend to be quite supportive of their wives’ contraceptive choices, even if very few men actually use a male method of birth control.
Indonesia is a mixture of more than a thousand ethnic groups speaking over 700 languages, living on over 6000 large and small islands. Fortunately, they are united by a single official language, although most Indonesians are multilingual. The motto of their National Family Planning Program is: “Realizing Quality Families”.
The country has supported family planning for decades. When we visited Bali (another Indonesian island) in 1996, we learned about banjars—the community organizations for a small village or neighborhood. The banjar serves perhaps 1,000 people, and helps its members through thick and thin. Banjar members organize religious ceremonies, dances, weddings and funerals. I was surprised to learn that each banjar also keeps track of every family’s fertility plan; the husband registers if his wife is trying to conceive, is pregnant or if they are using contraception. Although this would be considered an invasion of privacy in the USA, Balinese society does not have a problem with this openness.
The fertility rate in Bali is a bit above replacement, but is similar to the average for Indonesia. Sumatrans, on the other hand, tend to have larger families, averaging 2.5 children per woman. This is where vasectomy could really be helpful!
Only a tiny number of men in Indonesia have had vasectomies—just 3 per 1000 men. The vasectomy peak in that country was 30 years ago, with double that number. Unfortunately, this is true globally; the number of vasectomies has declined rather than increased. I am proud that the USA is one of two countries bucking that trend; the other is South Korea.
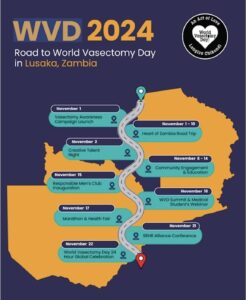
I know of two heroes who are working to change this trend—in addition to the vasectomy motivators in Sumatra. One is Dr. Charles Ochieng, whom I met at an international family planning meeting. He performs vasectomies, using the latest techniques, in his native Kenya. Another hero is Dr. Doug Stein, one of the co-founders of World Vasectomy Day (WVD). Trained as a urologist, Stein has limited his practice to male sterilization procedures. Each year he travels to a different country to train doctors there, and together they do a bunch of procedures—on WVD. This year it will be Zambia, November 24th. WVD is not just a day—in fact, they have 9 events scheduled in Zambia, all relating to vasectomy!
When I was practicing and a patient expressed an interest in being sterilized, I would suggest that vasectomy for her partner was safer and less expensive. I just read another, unfortunate statistic: 1 in 12 women will become pregnant within a decade after tubal ligation. To make things worse, many of these pregnancies will be in a Fallopian tube. A tubal pregnancy can cause serious—even fatal—bleeding.
I am happy that WVD, Dr. Ochieng and the vasectomy motivators in Sumatra are all promoting vasectomy. They are helping put the responsibility for family planning where more of it belongs—with men.
© Richard Grossman MD, 2024
